The Role of Pancreatic Elastase in the Diagnosis of Exocrine Pancreatic Insufficiency
Understanding Exocrine Pancreatic Insufficiency
Exocrine pancreatic insufficiency (EPI) involves the malabsorption of fats, proteins, and carbohydrates due to inadequate delivery of pancreatic enzymes that normally break down those fuels in the intestines.1 Symptoms of EPI can include bloating, abdominal pain, steatorrhea, vitamin deficiency, and weight loss.2 Particularly in children, delayed diagnosis of EPI can cause impaired growth. Early detection and treatment can minimize symptoms and prevent vitamin deficiency and malnutrition.3
Causes of EPI
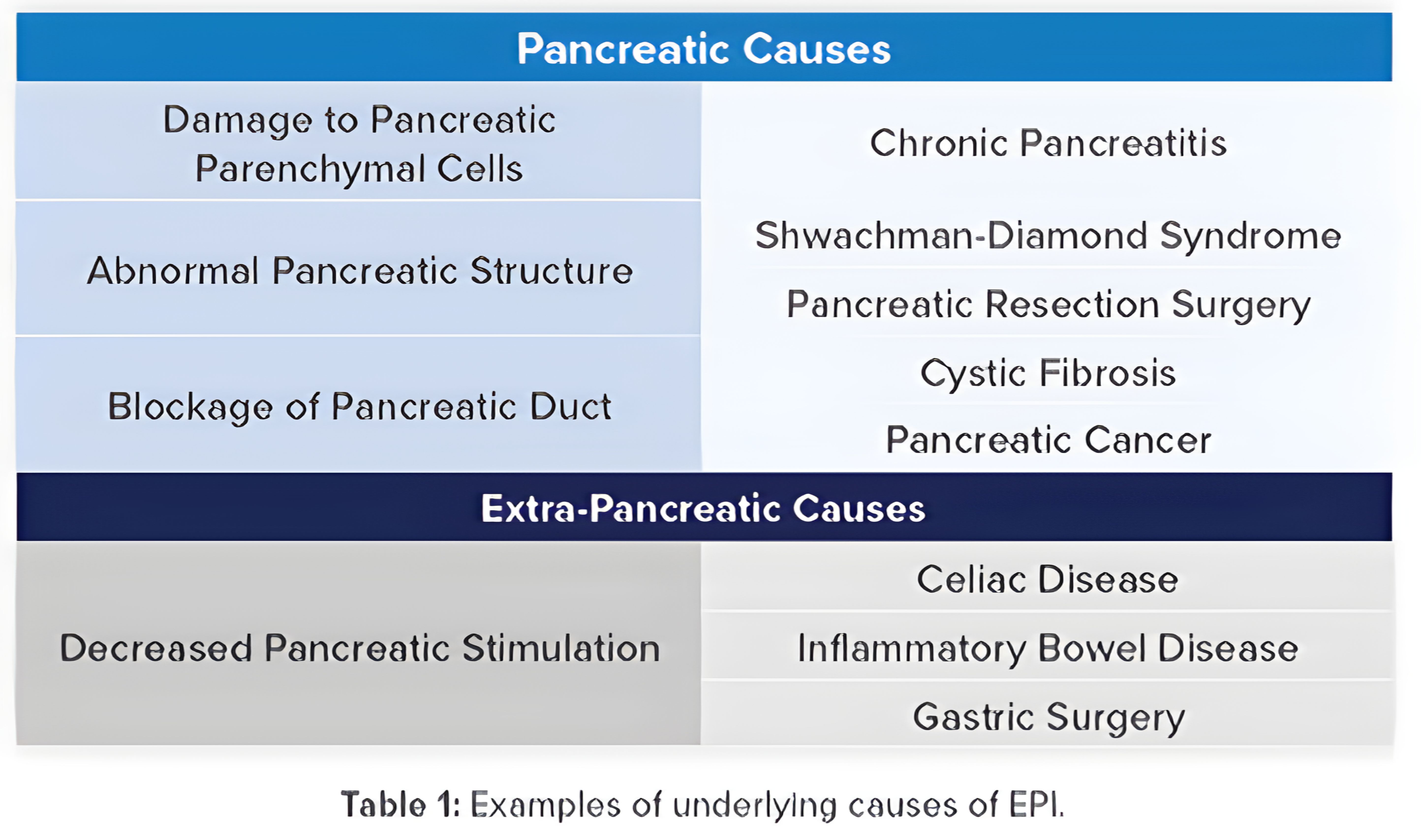
A wide range of diseases and disorders can lead to insufficient production, secretion, and/or function of pancreatic enzymes. The table (right) outlines some of the underlying pancreatic and extra-pancreatic causes of EPI, including chronic pancreatitis, cystic fibrosis, pancreatic cancer, and intestinal diseases that can affect signaling. 3,4
Methods for Diagnosing Exocrine Pancreatic Insufficiency
A variety of methods are currently used to assist with the diagnosis of EPI and their utility varies based on the underlying cause. Direct tests for pancreatic enzyme production are believed to be most effective for detection of mild pancreatic insufficiency, but they will not detect EPI caused by a decrease in intestinal signaling.3,4 Direct tests are also invasive, expensive, and rarely performed in the US. Some tests, including chymotrypsin and fecal fat, require a special diet and/or cessation of pancreatic enzyme replacement therapy (PERT) and daily stool collection. Issues with patient compliance often affect the accuracy of results. In addition, indications other than EPI, such as bile acid deficiency and diseases of the proximal small intestine, can cause high fecal fat levels.2,4-6 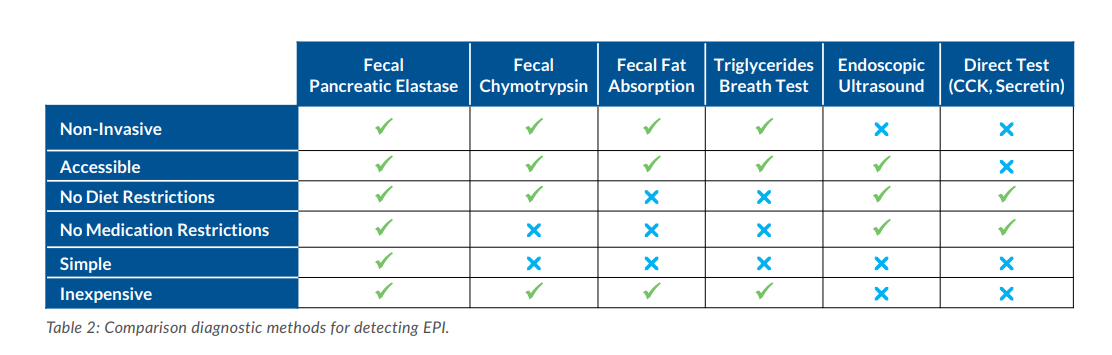
Pancreatic elastase (Elastase-1, PE-1, PE) refers to a family of digestive enzymes known as chymotrypsin-like elastases (CELAs) produced by acinar cells in the pancreas. The concentration of pancreatic elastase in fecal samples correlates well with overall pancreatic enzyme output. Unlike other tests for EPI, PE testing is non-invasive, widely available, reasonably priced, and doesn’t require diet or medication restrictions. Research has demonstrated that levels of PE below 200 μg/g are often indicative of EPI.2,7
Active Isoforms of Pancreatic Elastase
Due to a gene duplication, both the CELA3A and CELA3B isoforms of pancreatic elastase are active8. Using a proprietary CELA3Bspecific assay, ALPCO has demonstrated the variability in CELA3A vs. CELA3B production among normal subjects and the importance of strong measurement of both isoforms to avoid under-reporting of PE values. As seen in Graph 1 below, many normal individuals with no symptoms of EPI primarily express the CELA3A isoform. For these individuals, an assay with poor detection of CELA3A would erroneously report very low values of PE, triggering a suspicion of impaired pancreatic enzyme function. ALPCO utilizes a panel of samples containing both CELA3A and CELA3B isoforms of PE at concentrations spanning the AMR of the assay to ensure proper reporting of PE values from batch to batch.11 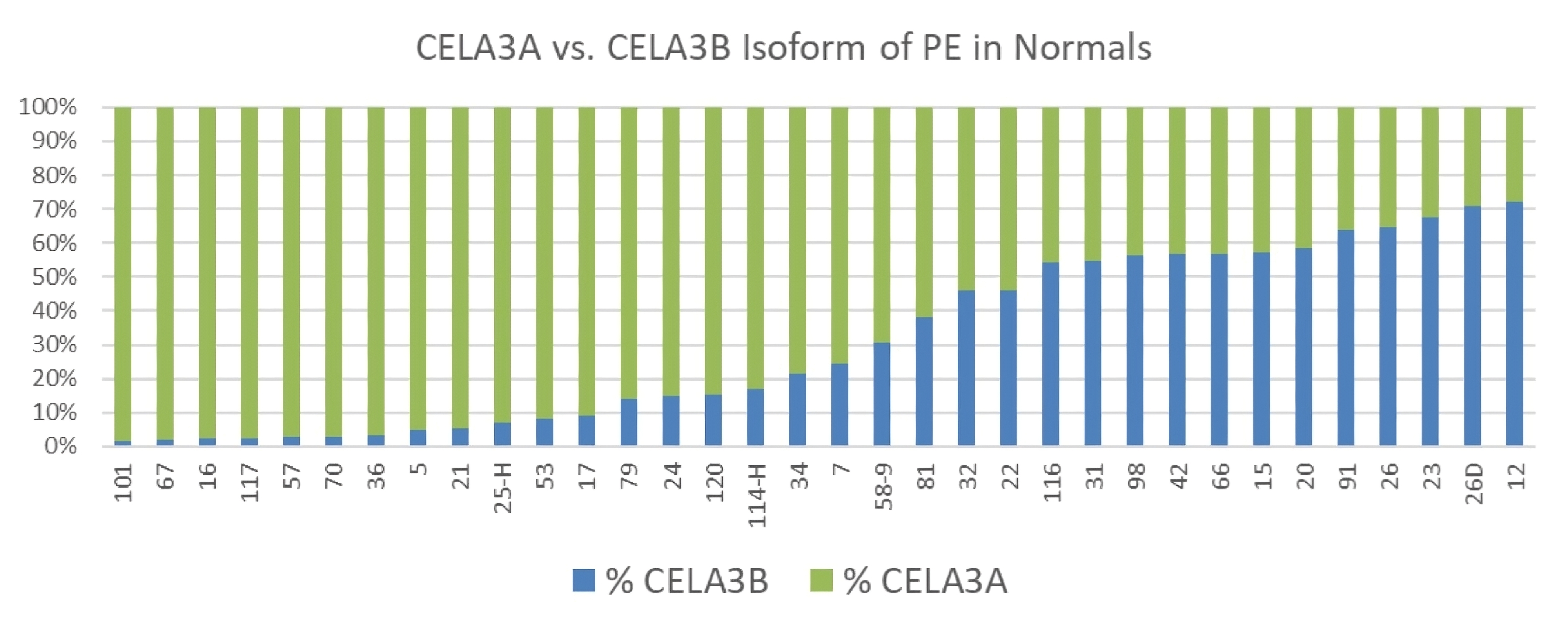
Graph 1: Distribution of CELA3A and CELA3B isoforms of PE in 34 normal individuals
Recommended Cut-Off(s) for PE in the Determination of EPI
Many manufacturers and reference laboratories involved with testing of fecal pancreatic elastase (fPE or PE) refer to levels above 200 μg/g being normal, between 100 and 200 μg/g indicating mild or moderate EPI, and below 100 μg/g indicating severe EPI. In practice, these levels have not stood up to scrutiny. Two recent systematic reviews and meta-analyses have demonstrated that a single cut-off of 200 μg/g is practical and sufficient to differentiate normal from patients with EPI (mild, moderate, or severe).9,10
In a study performed using the ScheBo ELISA for pancreatic elastase in 1996 and referenced in the ScheBo ELISA instructions for use, researchers clearly demonstrated that levels below 100 μg/g for PE were predominant in individuals with severe, moderate, and even mild EPI (Graph 2).11,12 Moreover, PE between 100-200 μg/g has been observed in patients with severe EPI.13

Thus, PE is not useful for categorizing EPI into mild, moderate, or severe categories. It is useful in identifying the presence or absence of EPI with a clinical sensitivity from the meta-analysis of 95%, 75%, and 54% for severe, moderate, and mild EPI, respectively, and a clinical specificity of 85%.9 The use of the 200 μg/g cut-off and the difficulty in detecting mild EPI are important for clinicians to understand when considering PE results and clinical symptoms to make treatment decisions.

Interpreting PE Results
There are several things to consider when interpreting PE results in the context of EPI. First, pancreatic enzyme production is closely linked to diet and nutrition. The amount of fat and protein in an individual’s diet can affect pancreatic enzyme levels and pancreatic elastase measurements, particularly in normal patients or those suspected of mild insufficiency. Long-chain fatty acids and certain essential amino acids produce a greater increase in pancreatic enzymes than other nutrients.14,15 Second, PE testing is only effective in identifying mild EPI in about 50% of cases.9 Lastly, impaired digestion, even in patients with mild or moderate enzyme insufficiency, can lead to a deficiency of micronutrients and fat-soluble vitamins such as D and K with associated clinical implications.16,17 PE values must be carefully considered in conjunction with diet and other clinical findings when making determinations regarding enzyme replacement therapy and/or vitamin supplementation in patients suspected of EPI.
References
- Jawaid and Forsmark (2019). Exocrine pancreatic insufficiency following acute pancreatitis: True association or EPI phenomenon? Digestive Diseases and Sciences. 64:1731-1733.
- Capurso, et al (2019). Exocrine pancreatic insufficiency: prevalence, diagnosis, and management, Clinical and Experimental Gastroenterology. 12:129-139.
- Sankararaman, et al (2019). Management of exocrine pancreatic insufficiency in children. Nutrition in Clinical Practice. 34(1)S27-S42.
- Drewes (2013). Diagnosis and treatment of pancreatic exocrine insufficiency. World Journal of Gastroenterology. 19(42): 7258-7266.
- Singh, et al (2017). Less common etiologies of exocrine pancreatic insufficiency. World Journal of Gastroenterology. 23(39): 7059-7076.
- Azer, et al [Updated 2020 May 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK541055/.
- Shandro, B.M., et al. (2018). Challenges in the management of pancreatic exocrine insufficiency. World J. Gastrointest. Pharmacol. Ther 2018 October 25; 9(5): 39-46.
- Párniczky, A., et al (2016). Genetic analysis of human chymotrypsin-like elastases 3A and 3B (CELA3A and CELA3B) to assess the role of complex formation between proelastases
and procarboxypeptidases in chronic pancreatitis. Int. J. Mol. Sci.17, 2148; doi:10.3390/ijms17122148 - Siegmunde, et al. (2004). Die diagnostische Validität nichtinvasiver Pankreasfunktionstests -- Eine Metaanalyse [The diagnostic validity of non-invasive pancreatic function tests--a meta-analysis]. Z Gastroenterol. 2004 Oct;42(10):1117-28. German. doi: 10.1055/s-2004-813604. PMID: 15508057.
- Vanga, R.R., et al. (2018). Diagnostic performance of measurement of fecal elastase-1 in detection of exocrine pancreatic insufficiency: systematic review and meta-analysis.Clinical Gastroenterology and Hepatology. 2018;16:1220-1228.
- Löser, Chr, et al. (1996). Faecal elastase 1: a novel, highly sensitive, and specific tubeless pancreatic function test. Gut. 39: 580-586.
- ScheBo® Pancreatic Elastase 1™ Instructions for Use, version 2022-07.
- Lüth, S. et al. (2001). Fecal Elastase-1 Determination: ”Gold Standard” of Indirect Pancreatic Function Tests? Scandinavian Journal of Gastroenterology, 36(10), 1092– 1099. https://doi.org/10.1080/003655201750422729
- Keller and Layer (2005). Human pancreatic exocrine response to nutrients in health and disease. Gut. 54(Suppl VI):vi1–vi28.
- Löhr, J.M. et al. (2016). Clinical and laboratory diagnosis of chronic pancreatitis. Pancreapedia. DOI: 10.3998/panc.2016.14.
- Klapdor, S., et al. (2012). Vitamin D status and per-oral vitamin D supplementation in patients suffering from chronic pancreatitis and pancreatic cancer disease. Anticancer Research. 32: 1991-1998. 10.
- Kroon, V.J., et al. (2022). Pancreatic exocrine insufficiency following pancreatoduodenectomy: A prospective bi-center study. Pancreatology.