
January 6, 2015
Bone Metabolism: The Cycle of Bone Growth and Resorption
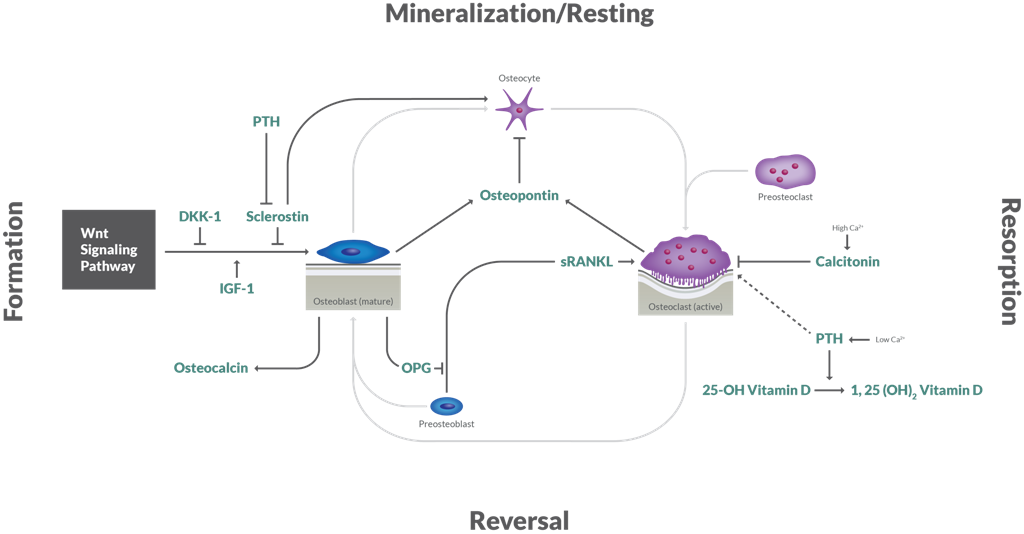 Bone metabolism is a continual cycle of bone growth and resorption that is carefully orchestrated by the dynamic relationship between osteoclasts, osteoblasts and an array of hormonal and regulatory influences. The relative levels of these signaling molecules dictate whether healthy, balanced bone metabolism ensues. Disturbances to this delicate equilibrium where resorption is greater than growth can weaken the skeletal architecture and put one at risk for the development of chronic and debilitating diseases such as Osteoporosis.
As we continue to gain a better understanding of the intricacies of bone metabolism and the key regulators involved, we may gain further insights into mechanisms underlying other bone-related diseases as well. ALPCO’s portfolio of bone metabolism assays serves as a powerful tool for studying bone-related pathologies and may help guide the development of new, targeted therapeutics.
Bone metabolism is a continual cycle of bone growth and resorption that is carefully orchestrated by the dynamic relationship between osteoclasts, osteoblasts and an array of hormonal and regulatory influences. The relative levels of these signaling molecules dictate whether healthy, balanced bone metabolism ensues. Disturbances to this delicate equilibrium where resorption is greater than growth can weaken the skeletal architecture and put one at risk for the development of chronic and debilitating diseases such as Osteoporosis.
As we continue to gain a better understanding of the intricacies of bone metabolism and the key regulators involved, we may gain further insights into mechanisms underlying other bone-related diseases as well. ALPCO’s portfolio of bone metabolism assays serves as a powerful tool for studying bone-related pathologies and may help guide the development of new, targeted therapeutics.
- Osteoporosis
- Osteopetrosis
- Paget's Disease
- Rheumatoid Arthritis
- Cancer & Bone Metastases
- Immobilization-induced Bone Loss
- Chronic Kidney Disease
Informational Videos
Introduction to Bone Biology
[embed]https://www.youtube.com/watch?v=inqWoakkiTc[/embed]Video produced by Amgen
Role of Osteoblasts & Osteoclasts in Bone Remodeling
[embed]https://www.youtube.com/watch?v=78RBpWSOl08[/embed]Video produced by Amgen
Role of OPG & sRANKL in Postmenopausal Osteoporosis
[embed]https://www.youtube.com/watch?v=VwCkyf0lQwo[/embed]Video produced by Amgen
Sclerostin: A Novel Regulator in the Cycle of Bone Growth and Resorption
Sclerostin, a protein product of the SOST gene, inhibits osteoblast activity via antagonism of the Wnt signaling pathway and plays a key role in the cycle of bone growth and resorption. Reports show that sclerostin expression and/or circulating levels are elevated in osteoporosis, immobilization-induced bone loss, rheumatoid arthritis, multiple myeloma and bone metastases, making it a therapeutic target of great interest for the fields of bone and cancer research.1,2,3 There are indications that sclerostin levels are also elevated with chronic kidney disease, suggesting relevance in the study of renal insufficiency as well.4,5 A growing body of evidence sheds light on sclerostin's novel role in the crosstalk between diabetes, obesity and bone metabolism. As the population continues to age, so does the prevalence of chronic diseases such as obesity, type 2 diabetes and osteoporosis. A number of recent reports have shown that sclerostin levels are increased and bone turnover markers decreased in type 2 diabetes.6,7,8,9 Type 2 diabetes is associated with increased fracture risk, and it appears that the Wnt signaling pathway may be intimately involved, potentially at the level of insulin secretion from the pancreatic beta cells. [embed]https://www.youtube.com/watch?v=ajsioxRrf1I[/embed]Video produced by Amgen